It’s urgent, the reason of false negative in COVID-19 nucleic acid test and its countermeasures!
Author: Hongge comes from Medical Wechat WeChat official account.
Recent epidemic situation in ChinaIn the process of getting up, there are some situations that deserve our attention.the most importantIsFalse negatives in nucleic acid detection. Intercepting relevant news, it was found that 8 confirmed patients in Shijiazhuang on the 22nd were repeatedly negative for nucleic acid detection, and 5 confirmed patients in Shijiazhuang on the 24th were repeatedly negative for nucleic acid detection.
On the 22nd, there were 11 new confirmed cases in Shijiazhuang, including:
Case 1: Male, 52 years old, from Huangjiazhuang Village. On the evening of 21st.Ninth nucleic acid positive;
Case 2: Male, 13 years old, Niujiazhuang Village. On the evening of the 21st.Nine times nucleic acid positive;
Case 3: Female, 11 years old, Zhongyao Village. On the evening of the 21st.Nine times nucleic acid positive;
Case 4: Male, 49 years old, Nanqiaozhai Village. On the evening of 21st.Ninth nucleic acid positive;
Case 5: Male, 47 years old, Niujiazhuang Village. On the evening of 21st.Ninth nucleic acid positive;
Case 6: Female, 65 years old, Niujiazhuang Village. On the evening of 21st.Ninth nucleic acid positive;
Case 7: Male, 11 years old, grandson of Case 6. On the evening of 21st.Ninth nucleic acid positive;
Case 11: Male, 67 years old, Xiaoguozhuang Village, husband of Case 2 on January 7th. On January 3, it was transferred to centralized isolation medical observation; On the evening of 21st.11th nucleic acid detectionFinally positive;
On the 24th, there were 7 new confirmed cases in Shijiazhuang:
Case 1: Female, 65 years old, Nanqiaozhai Village. Centralized isolation on the 11 th.Nucleic acid after 9 times, 22 positive.
Case 2: Female, 4 years old, Nanqiaozhai Village. Centralized isolation on the 11 th.Nucleic acid after 9 times, 22 positive.
Case 3: Female, 4 years old, Mi Jie, Chang ‘an District. Centralized isolation on the 13 th.Nucleic acid after 8 times, 23 positive.
Case 4: Female, 64 years old, Xiaoguozhuang Village. Centralized isolation on the 10 th.After 11 nucleic acids, 24 positive.
Case 5: Male, 34 years old, Xiaoguozhuang Village. Centralized isolation on the 8 th.After 11 nucleic acids, 24 positive.
Case 6: 34-year-old female, Liujiazuo Village, was positive for nucleic acid on the 5th, was diagnosed as asymptomatic infection on the 6th, and was clinically confirmed on the 24th.
Case 7: A 28-year-old male, living in Yuhua District, went to work by car at Zhengding Airport on weekdays. He was diagnosed as asymptomatic infected with nucleic acid on the 5th, and was clinically confirmed on the 24th.
Since the outbreak of COVID-19 last year, the topic of high false negative rate of nucleic acid detection has been the focus of attention. It has been reported that the positive rate of Covid-19 detection by fluorescence quantitative RT-PCR is only 30%-50% at present, which leads to extremely high false negative rate.
For Hongge, who doesn’t know much about the test, this paper analyzes the relatively high false negative test by searching articles and documents, and summarizes some reasons to discuss with you.
First, the incidence of COVID-19 suggests that it is highly possible to collect positive samples in a proper time.
Academician Yuan Guoyong’s team conducted this cohort study in Hong Kong Princess Margaret Hospital and Queen Mary Hospital. From January 22 to February 12, 2020, 23 hospitalized patients who were diagnosed as COVID-19 by laboratory examination of nasopharyngeal or sputum specimens were screened in the two hospitals.
A total of 173 respiratory specimens were collected from 23 patients. The researchers used RT-QCPR to determine the viral load in the samples. The results showed that the median viral load of respiratory tract samples was 5.2 log10 copies /mL (interquartile range was 4.1-7.0), and only 3 patients (13%) did not detect Covid-19 RNA in saliva samples.
The researchers observed that,The viral load in saliva was the highest in the first week after the patient developed symptoms, and then gradually decreased.Eight days after the patient developed symptoms, airway extracts were collected, and there was no obvious downward trend in viral load. Of the 21 patients who did not die,Seven people (33%) could still detect viral RNA after 20 days of symptoms, but this was not related to the severity of the disease.
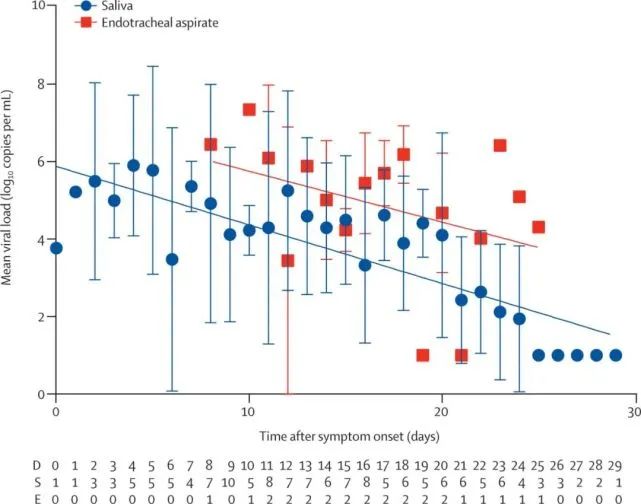
▲ Changes of viral load in saliva (blue line) and airway extract (red line) of all 23 patients. Abscissa D- days after symptoms appear; S/E- number of saliva/airway samples.
AprilAccording to a study published in Nature Medicine, COVID-19 patients are most infectious before symptoms appear, and they begin to shed SARS-CoV-2 2 2-3 days before the first symptoms appear.
https://doi.org/10.1038/s41591-020-0869-5
The study, led by Eric Lau of the University of Hong Kong, involved 94 patients with COVID-19 admitted to the Eighth People’s Hospital of Guangzhou, China, 50% of whom were male, with a median age of 47 years. Among them, 61 of 93 patients were mild. Specifically, the researchers collected the throat swabs of 94 COVID-19 patients who were treated in the Eighth People’s Hospital of Guangzhou, China from January 21st to February 14th. From the onset of symptoms to 23 days after onset, 414 throat swabs were collected.
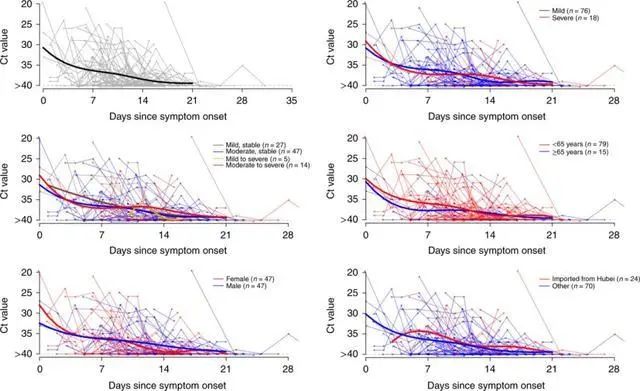
The results show that the researchers areThe high viral load was detected shortly after the patient developed symptoms, and then gradually decreased to the detection limit around the 21st day.There is no significant difference in viral load among different sexes, age groups and disease severity.
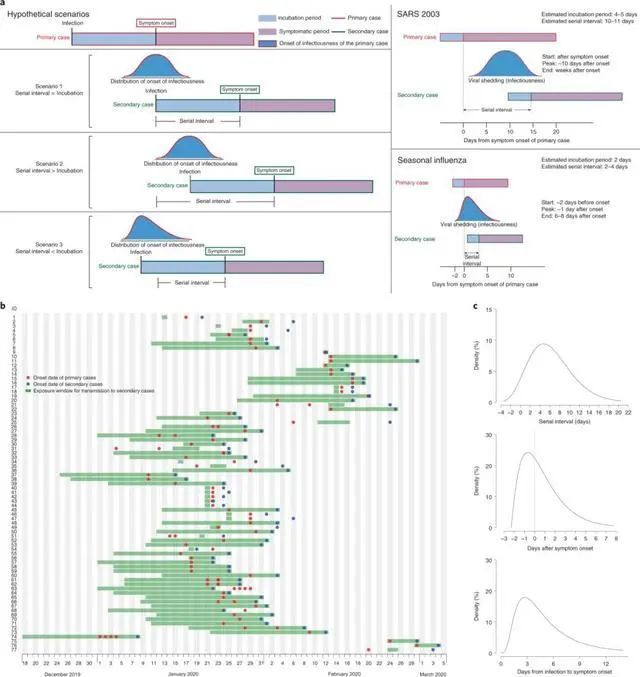
In addition, the researchers also analyzed 77 samples of "transmission pairs" from public data to assess how much time passed between the onset of symptoms in each patient. It assumes that the median incubation period (the time from infection to symptoms) is 5.2 days.The research team concluded that infectivity began 2.3 days before symptoms appeared, and peaked 0.7 days before symptoms appeared.
In the sensitivity analysis, the same estimation procedure is used, but assuming that the infectious attack is unchanged 1-7 days before the symptom occurs, thenIt was found that the infectivity reached its peak 0-2 days before the onset of symptoms, and the transmission ratio before the onset of symptoms was 46% to 55%.
The study also found that,The virus may start shedding 2-3 days before the first symptoms appear.After the symptoms appear, the viral load in the patient’s body decreases faster. This is consistent with the results of two recent studies. On April 1st, teams from Munich, Germany, Berlin and Cambridge, England published the article "Viro logical assessment of hospital patients with Covid-2019" on Nature. It was found that the shedding peak of Covid-19 occurred in the early upper respiratory tract infection.This shows that virus carriers may be the most infectious when they have mild symptoms or almost no obvious symptoms.
Brother Hong:From the above two documents, we can draw a conclusion that the virus shed and spread 2-3 days before the symptoms appear after infection, and after the symptoms appear, with the passage of time,The viral load of throat swab decreases gradually, and the viral load detected within 7 days after symptoms. If symptoms have existed for more than 20 days, the reliability of negative conclusion of throat swab is poor.
Solution:We need to publicize the law of the new crown to the people and medical workers, and improve our vigilance against COVID-19. It is best for patients to see a doctor in time, and doctors can also suspect this possibility. Only at the right time can we collect high-content samples and diagnose and control them in time.
Second, accurate sampling strategy is the best means to reduce false negative results.
In February, a study published by Medrxir, a pre-printed website, collected respiratory tract samples such as nasal swab, throat swab, sputum and bronchoalveolar lavage fluid (BALF) from patients diagnosed with COVID-19, and included 213 Covid-19-infected patients admitted to the Third People’s Hospital of Shenzhen from January 11th to February 3rd, 2020, who were diagnosed by Guangdong CDC. A total of 866 respiratory tract samples, including 490 nasal swabs, 205 throat swabs, 142 sputum samples and 29 BALF samples, were collected at the time of admission and after each time point. According to the collection date, the samples were divided into 0~7 days, 8~14 days and ≥15 days after onset. According to the guidelines on prevention and treatment of Covid-19 infection issued by National Health Commission, patients were divided into severe and mild cases.
Three groups were divided according to the sample collection time after onset, and the viral nucleic acid was quantitatively determined.The positive rate of viral nucleic acid in sputum samples was the highest in the group of 0~7 days after onset.The positive rates of severe and mild cases were 88.9% and 82.2% respectively.Followed by a nasal swab.(73.3% and 72.1% respectively),The throat swab again.(60.0% and 61.3% respectively). In mild cases, the positive rate of nasal swab and sputum samples is similar.
The positive rate of BLAF samples collected from 8 to 14 days after the onset of severe cases was 100%.However, the BALF samples of 3 mild cases were negative. In all cases, the positive rate of sputum samples was the highest in the 8~14 days after onset, which was much higher than that of nasal swab and throat swab. It is worth noting that the positive rate of throat swab in severe patients is only 50%, and that in mild patients is only 29.6%.
In the group ≥15 days after onset,The positive rates of BALF, sputum and nasal swab from severe cases were similar. In mild cases, the positive rate of sputum and nasal swab is similar, which is much higher than that of throat swab.
For the diagnosis of viral nucleic acid in COVID-19’s patients,Sputum samples are the most accurate, followed by nasal swabs. It is not recommended to collect throat swabs for diagnosis.
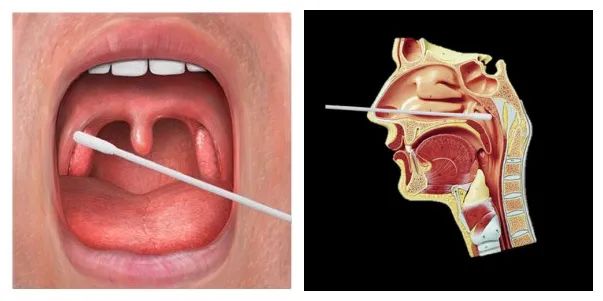
The difference between oropharyngeal swab and nasopharyngeal swab
anusswab
Brother Hong:
1. Oropharyngeal swab is the least painful and most acceptable, but it has to bear the consequences of high false negative results. My suggestion is to use it according to the epidemic risk in the first epidemic area.
2. The positive rate of nasopharyngeal swab is higher than that of oropharyngeal swab, which is why nasopharyngeal swab is introduced into laboratory examination in the fifth edition of Diagnosis and Treatment Plan for Pneumonia Infected by Covid-19 (the fourth edition is still pharyngeal swab). If we want to pursue accuracy, it is suggested to use it, or to use it when screening people in close contact or sub-close contact. At present, the examination of returnees in domestic reports seems to be nasopharyngeal swab method.
3. Alveolar lavage fluid can’t be used for screening in the general population, so it is suggested that hospitals with ICU should use it for screening severe pneumonia patients living in ICU for COVID-19 patients.
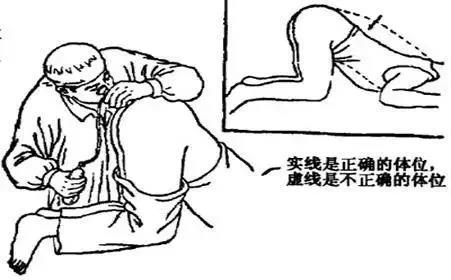
4. Deep expectoration seems to be the best sample, but many patients in COVID-19 have a dry cough, which may not be possible.
5、anusSwabs were used in Daxing epidemic in Beijing, which is the first time to use this method in the screening process. In some literatures,anusAlthough the positive rate of swabs is not high, as I remember, it seems to be more than 10%, but it does not seem to coincide with the patients with oropharyngeal swabs, suggesting that the virus may attack the gastrointestinal tract, and also suggesting that there may be the possibility of gastrointestinal transmission in Covid-19. Although the initial symptoms of some patients are gastrointestinal symptoms such as abdominal pain and diarrhea, there are also ACE2 receptors in the digestive tract, which is theoretically possible, but it has not been confirmed at present. So,anusMy suggestion is that swabs can only be used as a supplement to nasopharyngeal swabs, and it is better to select patients whose first symptoms are digestive tract symptoms more accurately, which is unlikely to be used as a means of large-scale screening.
Solution:It is best for National Health Commission to issue a guiding document for large-scale screening, and make detailed regulations on what population and what sampling methods to adopt under what circumstances.,When local governments encounter an outbreak in COVID-19, it’s best to ask professionals to act as consultants and make choices according to the actual situation.
Third, the consistency of sampling ability of sampling personnel affects the sampling results.
Garbage in, garbage out (garbage samples produce garbage results), which is a sentence that inspectors often say.
The sampling team is huge, and the ability of sampling personnel must be uneven. In addition, people may have such fears about sampling, which often leads to unqualified samples.
Generally, there is an internal standard in the molecular diagnostic reagent to monitor the detection process, for example, RNaseP is used as the internal standard. If both the sample response curve and the internal standard response curve displayed by the fluorescence PCR platform do not jump, it means that the quality of the collected samples may have problems or false negatives may occur due to improper experimental operation, which needs to attract the attention of medical workers. The RNaseP internal standard can monitor the sample collection and ensure the accuracy of the test results.
Note: RNaseP is ribonuclease P, which is one of the most important ribozymes in human body. It is ubiquitous in all organs, tissues and cells of human body, and can detect RNA nucleic acid fragments from human body samples, and can also be used as an internal standard.
And I privately asked the relevant person in charge of our city’s temporary inspection center. He told me that every day in our hospital, some samples were told that they needed to be re-sampled because the internal standard did not jump. Imagine that you didn’t wipe down a few cells in your throat swab collection, so will the negative of this nucleic acid be accurate?
Solution:Consistency training for nucleic acid sampling personnel will greatly reduce the human influence, and it is easier to standardize the sampling process by taking such sampling methods as nasopharyngeal swab. Our city seems to have trained the nucleic acid emergency sampling team very early. What about your city?
In addition, if in the environment of large-scale nucleic acid sampling, when testing under the standard of 5-mixed 1 and 10-mixed 1, according to the above principle of internal standard, it seems that there is no single-tube ability in the quality control of internal standard. Therefore, especially those in the emergency sampling team, we must pay attention to the standard sampling methods and remember to collect qualified samples as much as possible.
Fourth, choose the right oneSampling device
The virus preservation tube mainly consists of a sampling swab and a virus nucleic acid preservation tube (containing virus nucleic acid preservation solution). There are many kinds of virus preservation tubes on the market at present.It is very important for epidemic prevention and disease diagnosis to choose the appropriate virus preservation tube, reduce the infection risk of medical inspectors as much as possible, and keep the virus RNA stable without degradation..

The preservation solution UTM used in traditional virus collection tubes is based on Hank’s solution, with gentamicin, fungal antibiotics, BSA (V), cryoprotectant, biological buffer and amino acids added. Its main purpose is to maintain the virus activity within a certain temperature range, so that it is convenient for health and epidemic prevention departments to further isolate, culture and trace the virus and determine the pathogen. This kind of non-inactivated tube, which I call it, is good for further work, but the sameLive virus increases the infection risk of medical staff in the whole process of sample collection, transportation and testing!Personally, I think this kind of sampling tube for inactivated virus should be a better choice for disease control sampling.
And clinicalIn order to achieve the purpose of rapid detection, it is not necessary to cultivate the virus, but only to crack the virus, so as long as the integrity and stability of the virus nucleic acid can be guaranteed.nowCommonly known as inactivation tube.Many inactivation tubes in China are used.The inactivation component is guanidine salt, which is in this inactivation tube in our hospital.Guanidine salt can crack the virus, but it can’t protect the integrity of nucleic acid for a long time.The virus nucleic acid may have been degraded during the delivery of the sample to the laboratory, which will also cause a "false negative" in the detection. Many studies show that both temperature and time can affect the test results, so the COVID-19 Laboratory Testing Guide has clear requirements for samples to be tested within 24 hours after collection and transported at 4 degrees Celsius. If it is necessary to exceed 24 hours, it should be stored at -70 degrees Celsius.
And some manufacturers put forward another inactivation tube, a kind of.containNon-guanidine saltThe virus preservation tube containing protein denaturant can inactivate the virus and ensure the preservation of virus nucleic acid at room temperature.And the virus nucleic acid is stably stored for 7 days.Does not degrade.
Solution:
1, from sampling to testing, it is necessary to mark the time, so that quality control can be carried out on the preservation time, which is basically no problem in a better hospital.
2. For the front-line staff to do the corresponding training, they should know the advantages and disadvantages of various types of preservation tubes and adopt the best sampling tubes suitable for local conditions.
3. It is best for the country to recommend the selection of sampling tubes with the support of relevant experimental data.
5. Failure of reagents caused by virus mutation?
After the virus mutation in South Africa, Britain, Brazil and other places, there have been cases that turned positive after ten tests in various parts of the world, including China.The FDA recently warned that virus mutation has caused some reagents to fail, and listed several kits that may be affected by mutation. This means that virus mutation may have led to the failure of some nucleic acid detection or persistent false negative.
The FDA listed several kits that may be affected by mutation:
Accula SARS-Cov-2 detection (Mesa Biotech): If the virus mutates at the 28881st base (GGG to AAC), the detection of this kit will be affected;
TaqPath COVID-19 Combo Kit (Thermo Fisher Scientific): This kit detects three genes at the same time, and the variant B.1.1.7 appearing in Britain will affect one of the detection results;
Linea COVID-19 detection (Applied DNA Sciences): This kit detects two genes at the same time, and the variant B.1.1.7 appearing in Britain will affect one of the detection results;
Helix, an American company doing nucleic acid detection, also noticed the influence of virus mutation on detection. The company’s nucleic acid detection simultaneously detected three Covid-19 genes: ORF1ab, N, and S. Because the B.1.1.7 strain that appeared in Britain had deletion mutation in S gene, ORF1ab and N could be detected in the detection, but S gene could not be detected (4). This phenomenon is called "S gene withdrawal".
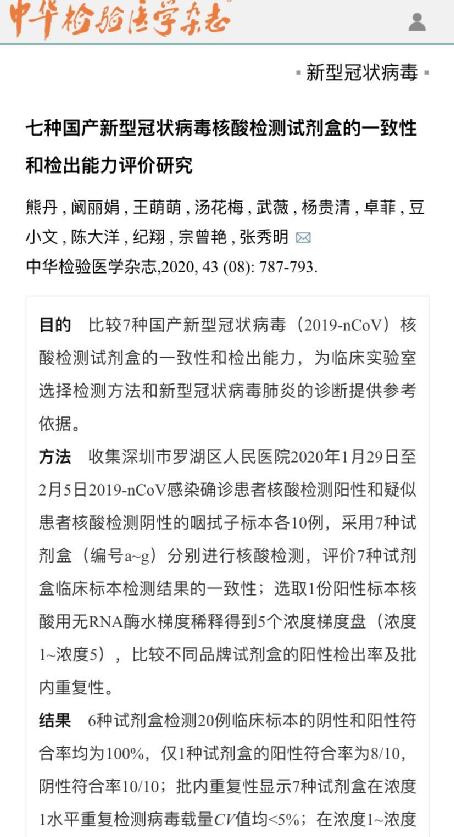
In addition, the sensitivity of reagents from different manufacturers to COVID-19 is different, and the country also organized a national evaluation of reagents last year. butIn an evaluation study on the consistency and detection ability of seven domestic novel coronavirus nucleic acid detection kits published by Chinese Journal of Laboratory Medicine in July, 2020, it was proposed that "some kits have poor detection ability for weakly positive samples,It is suggested that weak positive samples should be rechecked by kits from at least two manufacturers to ensure the accuracy of the results."
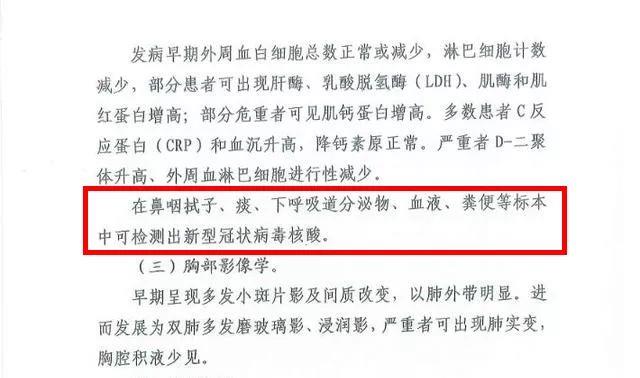
Several targets of nucleic acid detection in Covid-19 are ORF1ab gene, N gene and S gene.
In the Technical Guide for Laboratory Detection of Pneumonia Infected in novel coronavirus issued by China CDC (hereinafter referred to as the Technical Guide), the two targets of nucleic acid detection in Covid-19 are ORF1ab gene and N gene respectively.

On January 6th, the Weekly Report of China Center for Disease Control and Prevention published the results of gene sequencing analysis of two cases of Covid-19 infection in Shijiazhuang and Xingtai. According to the published results, the strain prevalent in Gaocheng, Hebei Province, is different from the strain found in other places in China recently, and is homologous to the strain reported in Russia last July, belonging to strain B.1.1.123
Coincidentally, the mutation happened at the 28881 ~ 28883 bases of the virus gene of this strain, and this is exactly the position of the forward primer of the N gene!
This also explains why there were many negative results at that time.
I guess this is one of the reasons why the criteria for judging nucleic acid positivity have also changed.The judgment position that the single target is still positive after retest is positive.
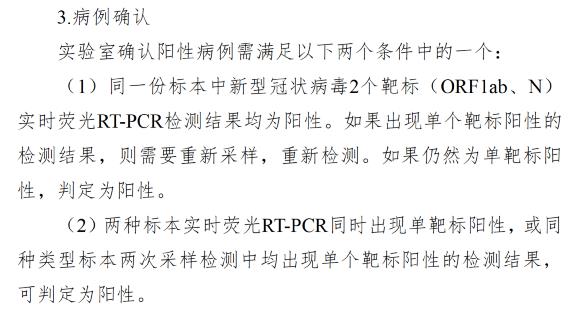
Figure/Current Criteria for Judging Positive Cases in Technical Guide
Solution:
1. Require manufacturers of nucleic acid reagents to conduct confirmatory experiments on the current mutant strains and propose technical solutions.
2, all localities should introduce at least two kinds of better quality detection reagents, for control use.
3. Information about the failure of test reagents that may be caused by mutated viruses should be effectively and widely reported in domestic laboratories.
Six, the standard implementation in the process of laboratory testing
the pastAccording to the guidelines issued by relevant institutions, the collected samples need to be inactivated at 56℃ before nucleic acid detection, which is very likely to degrade the Covid-19 nucleic acid, which will lead to the failure of normal detection and ultimately improve the false negative rate.In the early daysInactivation treatment is carried out for the sake of biological safety, to protect the staff engaged in testing from virus infection.
But later, there were many voices of doubt in the academic circles, becauseViral RNA is easily degraded by ribonuclease, because this enzyme has the highest activity at 60℃. Ribonuclease comes from two aspects, one is the sample cells, and the other is the foreign pollutants in the process of collection, preservation and transportation.
Last February, there was a similar research article.The high-temperature inactivation process before virus nucleic acid extraction significantly reduces the amount of detectable virus nucleic acid templates, which has been pre-published on the platform of scientific papers of China Academy of Sciences.
And last May,The Journal of Clinical Chemistry published the research of Chinese scholars on Covid-19’s false negative test.The study confirmed that,Thermal inactivation can cause the increase of Ct value reflected by PCR and cause false negative results.Specifically, 46.7%(7/15) of the weakly positive samples were false negative after inactivation (a surprising proportion). Another inactivation method is to inactivate the virus by dissolving the virus protein with guanidine hydrochloride. This study confirmed that guanidine hydrochloride had little effect on PCR reaction, and the false negative rate was low, although there was also a false negative rate of 13.3%(2/15).
Related address: https://academic.oup.com/clinchem/article/66/6/794/5815979
I also inquired whether there was a 56-degree inactivation step in the detection process of CDC in the United States. Although my English ability was poor, I didn’t see this step by machine translation.
Including some other documents retrieved, it is also very clear that 56-degree inactivation does have a great influence on weakly positive specimens.
No matter the Manual of Nucleic Acid Detection in Medical Institutions in novel coronavirus (Trial) on July 13th, 2020 or the Manual of Nucleic Acid Detection in Medical Institutions in novel coronavirus (Trial 2nd Edition) on December 30th, 2020, there are corresponding descriptions.For the laboratory that has been inactivated with the sampling tube containing guanidine salt, there is no need to inactivate at 56 degrees for 30 minutes.This is only true if non-inactivated sampling tubes are used.

However, I learned from the familiar laboratory leaders that this is not the case. Many laboratories still require samples to be pretreated at 56 degrees for 30 minutes regardless of whether the tubes are inactivated or not. I can understand that they are worried about hospital infection and laboratory exposure. But generally speaking, reducing the false negative rate, increasing the detection amount and taking corresponding measures to control the epidemic situation as soon as possible, I think the corresponding suggestions in the corresponding guidelines are also the best choice from the overall situation and supported by data.
Our laboratory should not control the occurrence of hospital sensation and laboratory exposure at the expense of reducing the detection rate, but should focus on stricter control of experimental steps, more cautious PPE wear and higher laboratory environment.
Solution:
1. It is suggested that the state give special instructions to laboratories at all levels on this matter.
2. It is suggested that the country should further study the preservation solution of sampling tubes, and if there is any preservation solution that can not reduce the detection rate at 56 degrees for 30 minutes, it can also be recommended.
The above zero zero always said a lot of points, mainly about how to reduce false negative conclusions, hoping to give you a reference.
It’s been many days since I wrote this afternoon, mainly considering Spring Festival travel rush. Although the scale of Spring Festival travel rush is reported to have dropped by more than 75% this year compared with previous years, the population flow is still very strong. We may face the rising trend of an epidemic after Spring Festival travel rush, and how to make the work better may be a more urgent need before us.